
Prof. Kittipan Rerkasem
Leg Vein Clinic Thailand
Seeing red or purple spider veins around the ankles, small blue veins on the skin, or bulging green varicose veins along the legs is very common—especially among people who stand or walk for long hours, women after pregnancy, individuals who are overweight, or those with a family history of venous disease.
However, what many people do not realize is that these visible veins are often not the true cause. The real problem usually lies deeper inside the venous system, where the naked eye cannot see.
To clarify the terminology, a varicose vein refers to a larger, bulging vein that is typically more than 3 millimeters in diameter and is usually caused by faulty valves, making the vein appear raised or twisted under the skin. In contrast, spider veins (telangiectasia) are very small red, blue, or purple veins that are generally less than 1 millimeter wide and lie close to the skin surface. These are mainly cosmetic and are not considered “varicose veins” in medical definition
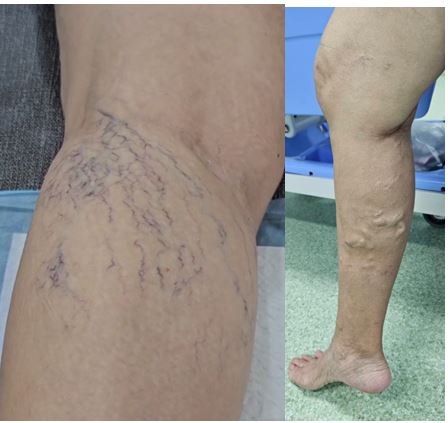
Left image shows spider vein (telangiectasia): Right image shows varicose vein
For a vascular specialist, the most important investigation before any treatment is Duplex Ultrasound (venous ultrasound).
This test accurately identifies whether the visible veins are caused by venous valve incompetence (venous reflux)—and precisely where the reflux originates, from the groin (saphenofemoral junction) down to below the knee, and from major veins such as the great saphenous vein (GSV) all the way to the tiny surface veins.
If the underlying source is not corrected, treating only the spider veins almost always results in poor improvement or rapid recurrence.
This article explains why every patient with spider veins or varicose veins should undergo a venous ultrasound before treatment, and why the concept of treating from the source (from A → Z) is the key to effective, long-lasting results.
- The Spider Veins You See… May Not Be the Real Problem
Spider veins (telangiectasia or “spider veins”) appear as fine red or blue lines under the skin. Many people view them as purely cosmetic.
In reality, a large proportion are caused by “downstream pressure” from reflux in deeper, larger veins.
A typical example:
- A patient sees spider veins around the ankles.
- Ultrasound shows GSV reflux from the groin all the way to the ankle.
- The backward pressure traveling down the leg causes the small veins to enlarge, bulge, and easily rupture.
Therefore, if one treats only the spider veins—for example with sclerotherapy or surface laser—without correcting the GSV reflux. The spider veins usually return quickly, often within 2–6 months. This is why venous specialists worldwide emphasize that
spider vein treatment should never begin without a duplex ultrasound.
- What Duplex Ultrasound Reveals: “Where and How Much Does It Reflux?”
A duplex ultrasound provides several crucial pieces of information:
(1) The exact location of venous reflux
Such as:
- Saphenofemoral junction (groin)
- Saphenopopliteal junction (behind the knee)
- Refluxing tributaries
- Incompetent perforator veins that feed the surface veins
(2) The length and extent of the incompetent vein
For example:
- Reflux from groin to ankle
- Or reflux only in a 15–20 cm segment of the thigh
This determines whether the patient needs endovenous laser, segmental ablation, or other targeted treatment.
(3) Excluding other conditions that mimic varicose veins
Such as:
- Deep vein obstruction
- Pelvic pain due to varicose vein congestion in pelviscso called pelvic congestion syndrome
Without identifying these, treating the surface veins alone may worsen symptoms or give incomplete results.
- The Key Principle: “Fix the Source, Not the Surface”
A fundamental principle in professional venous care is:
Treat from the source.
Just like trimming a tree:
- If you cut only the branches → they grow back.
- If you remove the root → the problem is solved.
In venous disease, the “root” is usually the GSV with faulty valves.
When these valves fail, high pressure is transmitted down the tributaries and into the spider veins, leading to bulging, discoloration, and visible web-like patterns.
Therefore, treatment must follow a systematic order:
Groin → GSV → tributaries → spider veins (A → Z)
If the sequence is correct, results are better and longer-lasting
After sealing the incompetent main vein—for example with laser treatment for GSV so called EVLA (endovenous laser ablation)—a common and remarkable observation is that:
Many spider veins naturally fade or disappear on their own, because the abnormal backward pressure has been removed. Conversely, starting with superficial injections or laser without addressing the deeper reflux yields only temporary improvement.
- Why Every Patient with varicose vein should Have an Ultrasound Before Treatment
Reason 1: To identify the true cause
The eye sees only the “result.”
Ultrasound reveals the “cause.”
Reason 2: To plan appropriate treatment
If a major vein is incompetent → treat with EVLA. If it is only superficial reflux → sclerotherapy may be sufficient.
Reason 3: To assess the severity
Ultrasound distinguishes between simple spider veins (C1) and hidden reflux in larger varicose veins (C2–C4), which may require comprehensive treatment.
Reason 4: To ensure the best and most durable results
Ultrasound-guided planning helps:
- Reduce recurrence
- Avoid unnecessary procedures
- Lower long-term costs
- Increase safety
Reason 5: It is the global standard of care
Major international guidelines—including the
- American Venous Forum (AVF)
- Society for Vascular Surgery (SVS)
- European Venous Forum (EVF)
all clearly state that
“Duplex Ultrasound is mandatory before treating any patient with varicose veins.”
- Do all patients with spider veins really need a duplex ultrasound before treatment?
According to international guidelines from the SVS/AVF/EVF, patients who have only small spider veins (telangiectasia) and no visible varicose veins do not always need a duplex ultrasound. However, all guidelines agree that an ultrasound should be done if there are signs that the spider veins may be caused by deeper vein reflux or varicose vein underneath. Warning signs include spider veins around the ankle (ankle flare), large reticular “feeder” veins, symptoms such as pain, heaviness, or burning, fast recurrence after previous treatment, or unusually widespread clusters of spider veins. These may indicate hidden reflux in larger veins like the GSV. Therefore, simple cosmetic spider veins usually do not require ultrasound, but if any of these warning signs are present, an ultrasound is recommended before treatment to ensure proper management and reduce the chance of recurrence, as emphasized in the guidelines.
- Summary: Treating from A to Z Is the Correct and Effective Approach
To truly and permanently treat varicose veins and spider veins, the treatment sequence must be correct:
- Start with duplex ultrasound to identify the underlying reflux
- Correct the incompetent major veins first (GSV)
- Then treat the tributaries and spider veins
- This produces the safest, most effective, and most durable results
Think of it as caring for a tree:
- Cutting only the leaves and branches allows the problem to return
- Removing the root solves it sustainably
Therefore, every patient with spider veins or varicose veins should undergo duplex ultrasound before starting any treatment to ensure the best outcomes and minimize recurrence.